Birth Should Not
Break Women.
Across Africa and the world, perineal trauma during vaginal birth is treated as inevitable. It is not. It's time to name the silence, the pain, and the cost of the "normal" birth experience and build something better.

The Scale of the Problem
0 Million
1Vaginal Births Annually
In Sub-Saharan Africa alone
The sheer volume makes perineal care one of the most impactful public health interventions possible.
> 0%
2Risk of Perineal Injury
During vaginal birth
The majority of women experience some form of tear. It is almost "expected" but it does not have to be.
4.5–7.5%
3Severe OASI Injuries
Obstetric Anal Sphincter Injuries
Sphincter damage leads to lifelong incontinence and is frequently underdiagnosed and poorly managed in low-resource settings.
Not all tears are equal.
Perineal injuries are classified by depth and involvement of surrounding structures. The degree determines treatment, recovery time, and long-term risk.
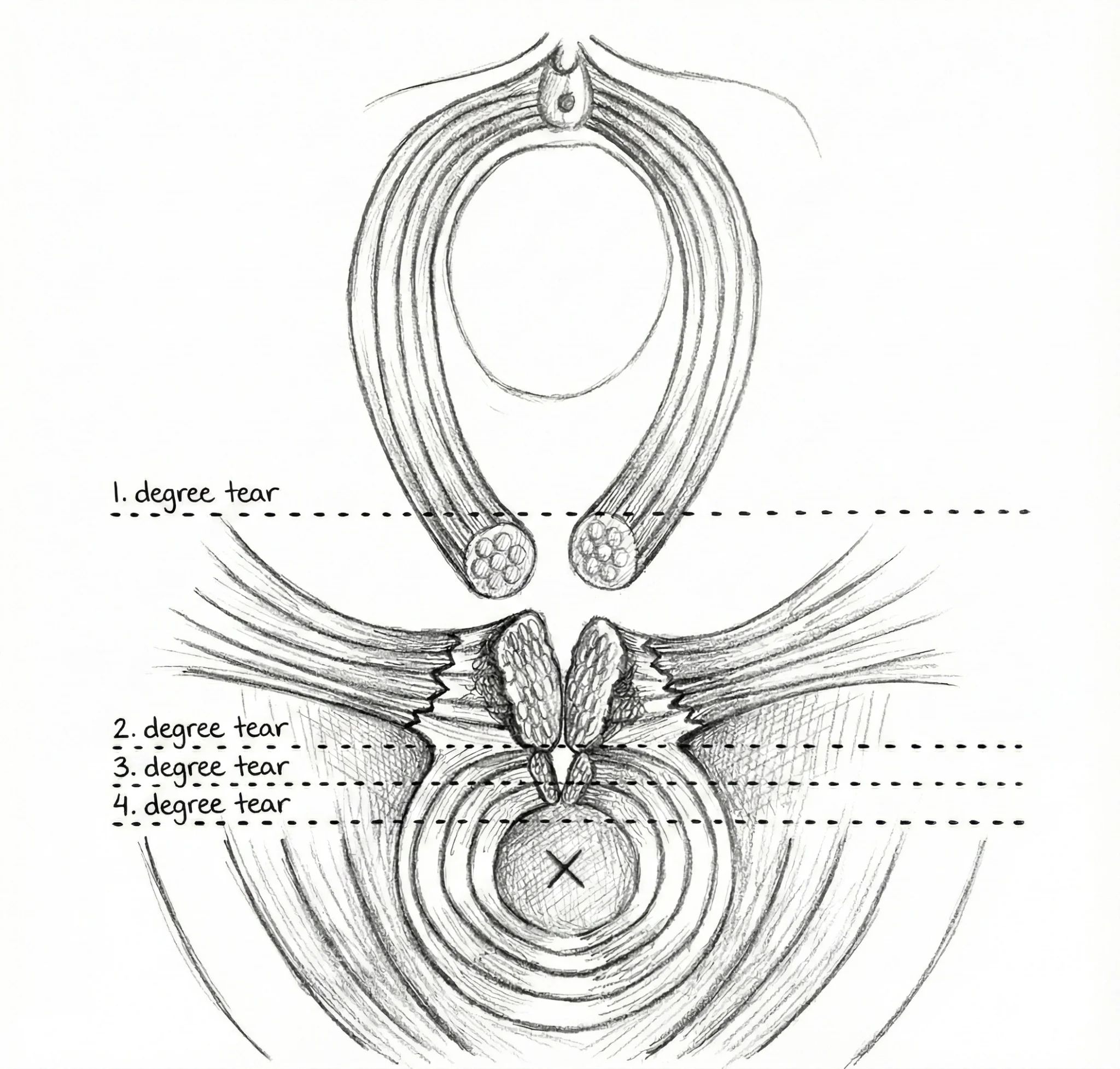
1st Degree: Superficial
Skin only: the fourchette and vaginal mucosa. Often heals without sutures.
2nd Degree: Into Muscle
Extends into the perineal muscle. Requires suturing. Most common surgical repair.
3rd Degree: Sphincter
Reaches the external anal sphincter. Risk of long-term incontinence.
4th Degree: Full Tear
Through both sphincters into the rectal mucosa. Highest severity with life-altering consequences.
The Physics of Crowning.
During the second stage of labor, the perineum must stretch to accommodate the fetal head. When this process is too fast, or when tissue is rigid, it fails under mechanical stress: in a predictable, preventable way.
Fast Descent4
When the baby descends rapidly, the perineum doesn't have time to stretch and thin naturally, causing explosive trauma. This is especially common in second deliveries, where the cervix dilates faster.
Tissue Inelasticity5
Age, scar tissue from previous repairs, inflammation, or simple inadequate preparation can make perineal tissue brittle: prone to snapping rather than stretching under load.
Absent or Inconsistent Support6
Without consistent Manual Perineal Support (MPS), mechanical tension concentrates at the weakest point: the posterior fourchette: and tears propagate along the path of least resistance.
The Episiotomy Paradox.
Episiotomy: a surgical incision to the perineum: was designed as a controlled, protective cut. In many African hospitals, it became a routine one. The evidence tells a more complicated story.
When performed freehand without a guide, at incorrect angles, or unnecessarily, episiotomy can increase severe injury risk by up to 20%.7
46 – 80%8
Pooled Episiotomy Rate in Africa
Compared to the WHO recommendation of 10% for selective, clinically indicated use only. This overuse indicates a lack of effective alternatives: not clinical necessity.
+ 0% Risk7
Extension Risk: Freehand Episiotomy
Poor cut angles (often toward the sphincter) cause the incision to extend into 3rd or 4th degree OASI territory. A controlled cut becomes an uncontrolled one.
45–60°9
The Correct Episiotomy Angle
Mediolateral episiotomy at the correct angle significantly reduces extension risk: yet most facilities perform it freehand with no guide and under time pressure.
7 Räisänen et al., BJOG, 2009. 8 Lawan et al., BMC Pregnancy & Childbirth, 2021. 9 Kalis et al., BJOG, 2012.
— Midwife, Kenyan Public Hospital, 2025
Support the ResearchWhat exists. Where it breaks.
Effective interventions exist in theory. The problem is consistent, reproducible delivery in the real world.

Manual Warm Compresses
Works: ~40% reduction in severe tears
Fails because: Requires a free hand, inconsistent temperature, midwife dependent: impossible to standardize in busy wards.

Manual Perineal Support (MPS)
Works: ~60% reduction in OASI rates
Fails because: Requires another free hand, varies enormously by clinician skill and attention: drops to near-zero efficacy when staff are overwhelmed.

Routine Episiotomy
Works: Intended to prevent uncontrolled tears
Fails because: Performed freehand in 46–80% of African births. Poor angles cause extensions into the anal sphincter: increasing severe injury risk by up to 20%.

Perineal Massage
Works: Some evidence of benefit in primiparous women
Fails because: Requires patient compliance antenatally, difficult to standardize, not practical during active crowning.
The gap is not in the science.
It's in the delivery.
We know what works. The challenge is making it simple, consistent, and reproducible: something any trained midwife can deliver reliably, every time, without an extra pair of hands.
See our SolutionA tear is never just a tear.
Perineal trauma triggers a cascade of consequences that touch the woman, her child, her community, and the entire health system.
The Woman10
- •Chronic perineal pain
- •Dyspareunia up to 2 years
- •Fecal / urinary incontinence
- •Post-partum depression
- •Stigma & loss of dignity
The Child11
- •Impaired early breastfeeding
- •Disrupted mother-infant bonding
- •Delayed developmental milestones
- •Reduced maternal responsiveness
The Economy12
- •Millions of workdays lost annually
- •Prolonged family caregiver burden
- •Healthcare re-visits and re-admissions
- •Long-term "invisible" economic drain
The Health System13
- •~1 hour of midwife time per 2nd° repair
- •Theatre resources for 3rd/4th° injuries
- •Suture material cost per repair: ~$33
- •Staff burnout in under-resourced wards
The data is clear.
The solution is overdue.
We believe birth should be a source of strength, not trauma. Meet the device we built to prove it.